Owing to this, it is believed that the tip of the catheter should be placed in the middle superior vena cava (SVC), outside the pericardial reflection enveloping the lower SVC. This corresponds to the level of the carina, ∼2 cm above the junction of the SVC and the right atrium (RA).
Where is a subclavian line inserted?
The infraclavicular approach is most common, and one of two skin insertion sites is used: either 1 to 2 cm inferior to the clavicle at the junction of its medial and middle thirds, or just inferior to the clavicle at its midpoint.
What surface anatomical landmarks are critical for guiding Infraclavicular subclavian catheterization?
What surface anatomical landmarks are critical for guiding infraclavicular subclavian catheterization? The midclavicular point and the lower border of the clavicle are critical for locating the subclavian vein for venipuncture.
How do you place a central line?
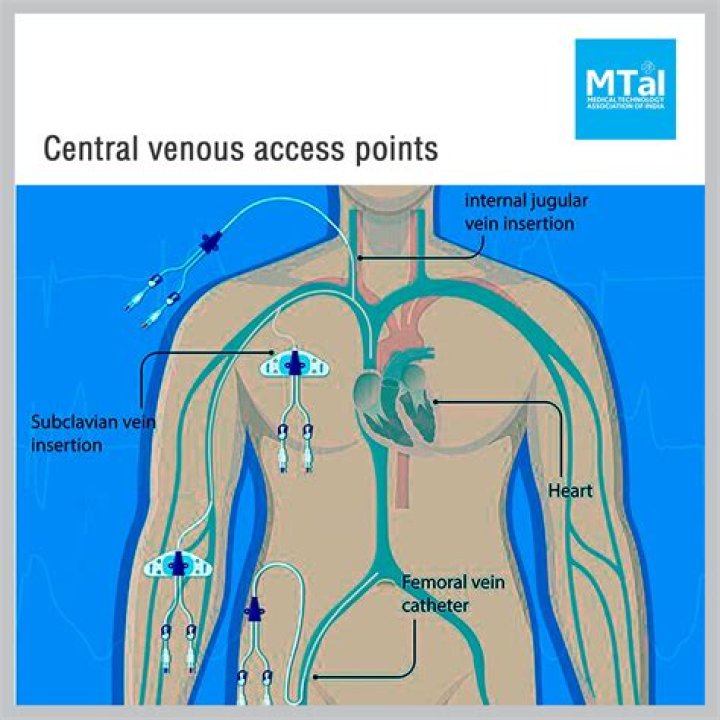
In order to insert a central line, the patient must be lying flat, and the area of the body where the central line will be inserted is exposed. The most common veins used for placement of a central line are the internal jugular in the neck, the subclavian vein near the clavicle, and the femoral vein in the groin.
How do you find the placement of a central line?
Confirming the position of the central venous catheter tip: For accurate CVP measurement, the tip of the central venous catheter (CVC) should lie within the superior vein cava (SVC), above its junction with the right atrium and parallel to the vessel walls 1.
Where should a central line be placed?
Insertion of a Central Line The most common veins used for placement of a central line are the internal jugular in the neck, the subclavian vein near the clavicle, and the femoral vein in the groin. The patient is covered, typically from head to toe, with a sterile drape.
What is subclavian central line?
Central catheters provide dependable intravenous access and enable hemodynamic monitoring and blood sampling [1-3]. The subclavian veins are an often favored site for central venous access, including tunneled catheters and subcutaneous ports for chemotherapy, prolonged antimicrobial therapy, and parenteral nutrition.
What is subclavian line?
The subclavian vein continues beneath the clavicle heading towards the sternal notch until at the medial border of the anterior scalene muscle it joins the internal jugular vein and becomes the brachiocephalic vein, also called the innominate vein.
Which of the following structures is used as a surface landmark when performing subclavian vein cannulation?
The subclavian vein can also be cannulated using a supraclavicular approach. This route is preferred by some authors. The essential landmark for the supraclavicular approach is the junction of the lateral border of the clavicular head of the sternocleidomastoid with the clavicle.
Does the subclavian approach reduce the risk of central venous line complications?
List of authors. Evidence suggests that the risk of major central venous line complications, particularly line-related bloodstream infections, is lower when the subclavian approach is used. This video will identify the landmarks and procedure for placement of a subclavian central line.
What is the target area of subclavian venipuncture?
This region of the vein is the intended target of subclavian venipuncture using the infraclavicular approach. The infraclavicular approach is most common, and one of two skin insertion sites is used: either 1 to 2 cm inferior to the clavicle at the junction of its medial and middle thirds, or just inferior to the clavicle at its midpoint.
How is a subclavian vein puncture performed?
In the Ultrasound Group, doppler was used to confirm the vein and a marker pen on the skin in front of the clavicle was made to indicate the direction of the subclavian vein puncture. ( See IMAGE BELOW). The rest of the procedure, including needle stick and catheter insertion was then performed similar to the Landmark Group.
What is the difference between left and right subclavian cannulation?
At the second site (clavicular midpoint), less effort is needed to maintain the shallow angle of insertion that keeps the needle in the coronal plane. Right subclavian cannulation, versus left, is sometimes preferred because it avoids the thoracic duct and because the right pleural apex is lower than the left.
